15.05.2025 - Update on Appendix 1.
appendix-1-new-15.05.2025.pdf (80.9 KB)
appendix-1-updated-15.05.2025.pdf (68.8 KB)
15.05.2025 - Update on Appendix 1.
appendix-1-new-15.05.2025.pdf (80.9 KB)
appendix-1-updated-15.05.2025.pdf (68.8 KB)
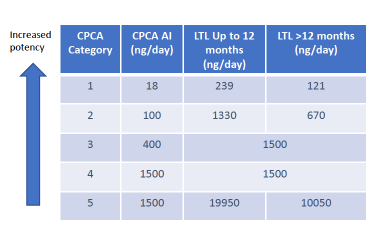
Do we have more insights on the remark “CPCA derived AI as substance tested positive in in vivo mutagenicity study. LTL cannot be applied and the AI will be capped at 1500 ng” linked to N-nitroso-ketamine?
It is not clear if this is in the ICH M7 sense or in the sense of Q&A 22 (or a combination of both).
In the previous version this remark was still: “LTL cannot be applied and the AI will be capped at 1500ng as the substance tested positive in in vivo and in vitro mutagenicity studies”
On the other hand, for N-nitroso-sertraline (CPCA category 2) it says “CPCA derived AI as substance tested positive in in vivo mutagenicity study”.
There are no remarks on LTL usage or LTL capping. But Q&A 22 LTL would mean 670 or 1330 ng/day anyway.
(So in vivo positive is impacting the Q&A 22 capping rules only? But generally for positive in CPCA category 5 or based on exact data and can there be other LTL limitations coming from in vivo positives?)
That’s an interesting point. I excerpted the 14 nitrosamines with in vivo positive results from the AI list. N-nitroso-ketamine is the only nitrosamine with CPCA category 5. The other 13 nitrosamines will be capped at 1500ng/day (or not capped due to the low acceptable intakes), even if LTL is applied. I think the EMA is trying to suggest introducing a cap on LTL for in vivo positive nitrosamines here.
I hope the guidance will provide clear rules on setting AI for in vivo positive nitrosamines in the future.
appendix-1-rev.9_in vivo positive.pdf (220.5 KB)
I’m just not sure if they intend the cap explicitly only for CPCA category 5 cases and if the cap remains 1500 ng/day (e.g. CPCA category 4 in vivo positive can still benefit from LTL up to 1500 ng/day or also no LTL possible?) and what this capping will mean if we have a true LTL for nitrosamines in the future (still looking back to CPCA to determine your access to LTL - will the LTL factors be constant across CPCA classes?)?
Also is it now for once “innocent until proven guilty” (whereas for nitrosamines it is often the reverse): you can use LTL on CPCA category 5 till the day of an in vivo positive - or CPCA category 5 doesn’t generally get its no cap anymore?
I assume N-nitroso-ketamine case might flag a flaw of CPCA (possibly putting too much attention on hydrogen scores and too little on overall structures). Yes, it is CPCA category 5, but there is probably a specific mechanism and an important role for conjugation/deconjugation influencing the distribution and therefore influencing the eventual effect (assuming it is still nitroso-typical).
Would be useful to investigate N-nitroso-ketamine mechanism and if and how CPCA misreasons on this compound rather than moving focus to LTL. Precaution (capping) is easy, mechanistic understanding is difficult and needed.
Thanks Eleni for sharing.
However, appendix-1 list for Ketamine, Nebivolol and Vanzacaftor molecules were updated on July 2023 and September 2024.
Can you please tell is this updated on 15-May-2025 ?
Dear Pooja
I prepared a doc for further clarification. hope it helps.
appendix-1-updates-comp-feb2025-may2025.pdf (50.0 KB)
Thanks Eleni for the clarification.
Dear Wybon,
‘‘Would be useful to investigate N-nitroso-ketamine mechanism and if and how CPCA misreasons on this compound rather than moving focus to LTL.’’
i am totally agree with you, this should be the main point of investigation due to Ketamine case.
But it should be answered clearly from the EMA which is the reason for not accepting the LTL approach for a drug with a clear short-term duration therapy drug.
kind regards
Christos
Capping is effective for CPCA Categories 3 and 4. The distinction between Category 4 and Category 5 is unclear; however, since the LTL approach can be applied to nitrosamines that test negative in in vitro assays, Category 5 may be regarded as equivalent to non-mutagenic nitrosamines. In this context, nitrosamines classified as Category 5 but showing positive results in in vivo studies no longer appear to be treated as true Category 5 compounds.
Regarding “innocent until proven guilty,” I recall that the AI for N-nitroso-sertraline was revised from 1500 ng/day to 100 ng/day following positive in vivo results. Prior to the increase to 1500 ng/day, the AI had been set at 100 ng/day. New data supersedes old data.
Therefore, it can be assumed that the LTL approach may be applied to CPCA Category 5 compounds up until the point when a positive in vivo result is observed.
These are conservative approaches, and I think it would be better to resolve them through chemical arguments, as you say. I am curious about the potency of N-nitroso-ketamine in in vivo tests.
This is what I would find strange as a general rule (without even considering the AI the in vivo data suggests) (scientifically and from a legal certainty perspective), especially considering the regulators motivation for the capping of the LTL per 7 December 2023 NIOG meeting was the uncertainty on the characterisation of the risk (CPCA-AI higher than real-AI (due to design mistake CPCA) and making this worse with LTL factors; reference example at the time N-nitroso-propranolol), not the fact that LTL would only be appropriate for non-mutagenic substances (actually unlikely alpha-hydroxylation risk is more correct, category 5 is not officially the non-mutagenic class).
Lack of LTL capping for CPCA category 5 was originally:
CPCA category 5 we treat differently in allowing the LTL because we think these are substances are very unlikely to be mutagenic. - per 7 December 2023 NIOG meeting
If now CPCA category 5 is treated the same like for example a CPCA category 4 (because unlikely mutagenic doesn’t apply anymore), you can revert back to the original motivation for the capping:
CPCA-AI higher than real-AI (due to design mistake CPCA) and making this worse with LTL factors, uncertainty about the real AI.
But this lack of characterisation of the risk isn’t the case anymore if in vivo data is presented?
Even if you stay at CPCA limits because in vivo quantitative use is not a regulatory option for now, you can still compare the CPCA-AI with the in vivo data to make a judgement call if CPCA is likely to underestimate the potency or not? (As a value, not as the text used to describe the class.)
Let’s for example assume N-nitroso-piperidine was an unknown “NDSRI”, it would be then CPCA category 3, 400 ng/day. But you get a LTL factor 6.7 temporarily with capping to 1500 ng/day, so 1500 ng/day is the limit.
Then you get in vivo data in on N-nitroso-piperidine, supporting an AI of around 1300 ng/day (or 8710 ng/day with LTL 6.7) (e.g. the NPIP in vivo mutagenicity data of Powley 2024 or Roper 2025 or the carci data of Gray 1991 is “new”) and the consequence is that the limit is now 400 ng/day without LTL or that the LTL limit just stays 1500 ng/day. When you knew less about the risk you could apply relatively a higher correction factor for LTL than when the risk was characterised, this is strange - especially considering lack of characterisation was the motivating for capping.
Even more strange when you have a real less-than-lifetime application.
Of course assuming the “real AI” of N-nitroso-ketamine is higher than around 200 ng/day (would be surprising if it isn’t?).
Remarkably in the meantime Table 3 of FDA is showing signs that in vivo positive data is being weighted to make temporary limit decisions (e.g. N-nitroso-fluoxetine).
I may not fully understand your thoughts, but I believe there are two basic rules.
When Eli Lilly proposed an AI of 4400 ng/day (or 1500 ng/day) for N-nitroso-atomoxetine, PMDA did not accept it. The reason was that, according to the M7 Q&As, the endpoint of in vivo gene mutation assays is mutation, not carcinogenicity, and currently, it has not been validated whether these assays alone can directly assess carcinogenic risk. At least for now, the results of in vivo studies appear to be used solely as a criterion for the presence or absence of mutagenicity.
The capping seems necessary for the case of N-nitroso-piperidine. When in vivo positive data become available, LTL is still considered valid and capping is done(1500 ng/day). When carcinogenicity data become available, the AI will be 1300 ng/day, but since it is below 1500 ng/day, capping will probably be done(1500 ng/day).
If in vivo studies are negative, or if cancer studies suggest an AI higher than 1500 ng/day, authorities may permit the use of an uncapped LTL value.
It seems strange to me that the LTL approach for nitrosamines is handled differently from the ICH M7 guidelines. But I expect this will be clarified when nitrosamines are formally included in ICH M7.
Why necessary for NPIP? Mutagenesis is the initiating event for nitrosamine-related carcinogenicity and if it is about redesigning the LTL-factors, we are also not doing this yet for the CPCA category 1 or 2.
NPIP BMDL50 from 2 TGR assays on NPIP (Roper 2025, Powley 2024): 2.3 mg/kg bw/day and 1.89 mg/kg bw/day.
If you would extrapolate those directly: 1890-2300 ng/day (mutagenicity endpoint, Jolly 2024 method). (This indeed what PMDA did not accept).
If you would potency rank to NDMA or NDEA (so make into a prediction of an AI for an acceptably low human cancer risk): 864-1051 ng/day (via NDMA, Lynch 2024 see Roper 2025), 501-610 ng/day (via NDEA, Bercu 2023, Zhang 2023, see Roper 2025). (Other calculations options can be proposed as well.)
All these values are the same order of magnitude than 1300 ng/day from actual carcinogenicity study on NPIP, so the extrapolation works, and why then not put an uncapped LTL to that? Or at least allow uncapped LTL on the CPCA category 400 (whereas 400 x 6.7 = 2680 ng/day only includes doubling compared to the real AI).
(That for NPIP 1300 ng/day becomes confirmed, shows that 2680 ng/day LTL usage was not a problem.)
So, if you would use the in vivo mutagenicity data not fully quantitatively (if this is not allowed) but just for a confirmation of the need for LTL restrictions on the CPCA limit (on maximum value or on temporarility of the limit) on CPCA?
I think this would be an elegant solution in fact, if LTL capping or LTL temporary use (for short term duration products) can be reconsidered already based on in vivo data, buying time to finalise the design of a regulatory framework allowing quantitative use of in vivo data, while not impacting product supply with in vivo data already on the table.
For the PMDA case you cite, I think you have to make a distinction between non-acceptance of in vivo mutagenicity data in any use or non-acceptance of direct calculation of an AI from in vivo TGR assay BMDL50 (4.4 mg/kg bw/day for N-nitroso-atomoxetine to 4400 ng/day, Jolly 2024), whereas other calculation options are possible (see for example Zhang 2025, Roper 2025, MfE position paper). It is not because 4400 ng/day is not accepted that the door is fully closed on the valorisation of in vivo data.
As I mentioned, remarkably in the meantime Table 3 of FDA is showing signs that in vivo positive data is being weighted to make temporary limit decisions (e.g. N-nitroso-fluoxetine). Without recognition of at least some aspects of Jolly 2024, I don’t see how 7200 ng/day can be published as interim limit for N-nitroso-fluoxetine.
Hi,
Can we apply LTL approach as per new EMA updates for N-nitroso betahistine which listed category 1, AI is 18 ng/day and positive in Ames test
@Yosukemino The Applicability of LTL is under consideration for the M7 revision; however, as of today, it can be used at the sole discretion of the agencies. I do not encourage using LTL just because it was used in another impurity. There has to be enough evidence to justify or propose it. The only exception to this rule seems to be clinical development.
There is a big unanswered question: Is the Carcinogenic potency of nitrosamines a function of total dose or of daily dose?
Thank you for asking, Abhijeet. As Naiffer explained above, LTL can be used under EMA Q22 in Q&A when permitted by agencies. The Ames positive result is unlikely to affect the LTL application.
FDA appears to be setting interim limits in a way other than LTL.
Thank you for sharing information, Naiffer. I have never heard cases of LTL application for nitrosamines in clinical development. It is a flexible approach.
I am not sure if this answers your question, but when we think about the mutagenicity of a compound, we say that there is no threshold for toxicity. Therefore, we set the daily acceptable limit so that the cancer risk is less than 1 in 100,000 even if we take it every day for 70 years. Roughly speaking, under Haber’s law, short-term high exposure and long-term low exposure are considered the same. However, because of the risk of carcinogenicity due to cytotoxic effects at high concentrations, authorities are reportedly cautious about applying LTL to nitrosamines. Thus, there are risks associated with high exposure to nitrosamines that are not yet fully understood.
Thanks …@Yosukemino and @Naiffer_Host
Hi Everyone! I would have a question regarding the “N-nitroso-tizanidine” impurity. We have not been able to find a standard for this compound and I was wondering if there is any evidence if this impurity can be formed. According to our knowledge, N-nitroso-tizanidine impurity 3 would form instead. We have also been able to collect two non-feasibility reports, yet these have not been accepted by the authority.
I would really appreciate your input, as we have not been able to find any literature on this compound. Could this be a similar case as with N-nitroso-amlodipine?
Thanks!
Synthesis of N-Nitroso Tizanidine is not possible.