Recently, it got to our attention that several NDSRIs indicated in EMA Appendix 1 theoretically could be in transdermal formulations (i.e., Rotigotine, Lidocaine, Methylphenidate etc.). with NDSRIs in Category 1, 2, 3 or more. Under EMA/409815/2020 there is no difference between route of administration unless you provide data.
There is a lot of uncertainty for nitrosamines, in comparison with elemental impurities where even correction factors for different routes of administration are present, and of course the corresponding tox. studies behind.
Considering the pharmaceutical form, it is our understanding that the risk should be less than oral ingestion, as the skin is considered a barrier. But, assuming NDSRIs content is on meaningful levels on the finished product, the following has been given a thought at least:
NDSRIs are commonly more hydrophilic than its parent API (higher logD at ph 5.5. of skin). The % of absorption of the API can´t be considered. Therefore, maybe evulating the quantity of nitrosamine actually released from the patch?
Perform an Ames test to determine if the NDSRI is -tive or +tive with or w/o S9 mix.
If it is positive only w/ S9, could metabolism happen on skin with an enzyme that convert the nitrosamine to a mutagenic metabolite?
If it is positive only w/o S9 or w and w/o S9, may local acummulation be an issue?
Maybe -tive an a higher limit could be applied after acceptance.
Depending on the outcome of the Ames an OECD 428 test could be considered? Is our understanding that anything in-vitro is better than in-vivo to avoid the particularities of a living being and the need of a PhD. Nonetheless, any % of absorption is better than the defaul 100%
Any other experimental options e.g., PK/TK studies?
Considering NDSRIs are controlled in ppb levels, we see a possible real challengue to actually detect anything in the bloodstream of the selected mamallian by the moment the sample is taken.
Have the community got the chance to work on this kind of pharmaceutical forms? Any suggestion? Very broad questions here, but any insight is highly appreciated.
By the way, kind of interesting. I wonder also about how to calculate the maximum daily dose. API quantity on the patch/day, API quantity released/day or API quantity absorbed/day.
This is a very tough topic. People have asked me, even with creams and ointments. There are some nitrosamines (smaller ones) for which some data is available for absorption from skin, though not always dependable. But with the NDSRIs, I think the data is really not available. Thus the agencies have decided to keep the same values for all routes of administration. The MDDs may be more for these formulations, which may be another challenge. Please remember that the limits determined by CPCA or any other mode are applicable to the finished product, so the onus will also be on the API manufacturers to anticipate all dosage forms and find a suitable limit. What a tangled web
Thank you for sharing this information and your thoughts on using NDSRIs in transdermal patches. It’s an interesting consideration, and I appreciate your proactive approach to assessing potential risks, particularly regarding nitrosamines. I’ll definitely look into this further and see if I can provide any insights or suggestions. Thanks again for reaching out!
I understand this approach for patches, where an MDD can be set even if it is not the actual amount of product absorbed. But how to estimate the MDD in a topical cream where the amount to be applied is not established?
Usually, most regulatory agencies ask for an MDD for a drug, no matter what the route of administration is and all impurity limits are calculated based on the MDD. So, you will need to find the MDD of your drug product before you do any calculations for impurities. If you are in generic, read the label of the RLD, if you are developing a new drug, find out what amoutn is being applied. Also, as unfortunate as it is, for transdermals, when we talk of impurities, we consider the absorption to be 100% unless otherwise proven.
From my experience, I think the worst-case approach is available for transdermal products. The conservative maximum application amount can be determined based on the symptoms and the size of the affected area. It’s the same as ICH Q3A, Q3B, Q3D, and M7.
@Jaume_Tomas
This is a question that we also had to discuss. In the case of creams or other topical applications with a “classic” API, the calculation may easily be made using its MDD. It becomes more difficult when it comes to a medicinal product without such an active ingredient (e.g. those with atypical active ingredients or homeopathic medicinal products). In this case, we used the finger tip unit (FTU) and calculated the worst-case application quantity on the whole body. This led to a MDD of 25 g of cream per application. So far there have been no queries from the (European) authorities…
Hi Naiffer, @Naiffer_Host
Sharing link to a recorded session on Analytical testing aspects of Nitrosamines in dermal products.
In this Presentation, Emiliano de Dominicis from Merieux provides an insightful analysis through case studies about work done on Benzidamine and Diclofenac active & Topical dosage forms, the focus here has been on Ointments/gels that are extensively used as NSAIDs. This work is being done in Europe, it would be worth understanding if a similar work specific to Transdermal patches is being evaluated. It will perhaps bring more Insights/perspective on this topic
Hi,
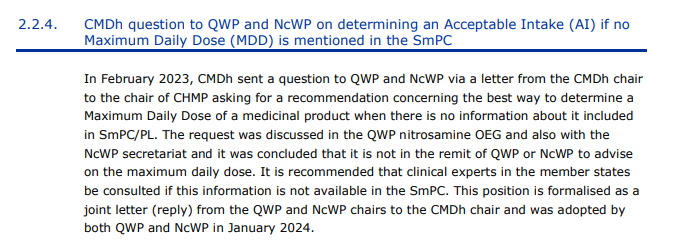
While reviewing the minutes of the last CHMP meeting, I found information that may be related to this topic. In the absence of information on MDD at SmPC, it is recommended to consult clinical experts in Member States to determine the maximum daily dose.
The citations are specifically for NDMA and N-nitroso-N-methyldodecylamine I believe, so the comments above on limited data availability remain valid I believe.
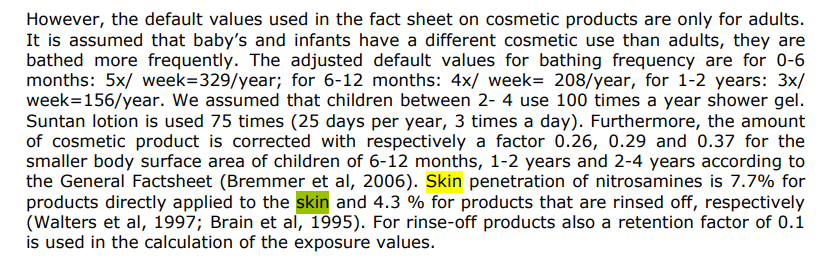
Molecule size, hydrophilicity and volatility of the nitrosamine are important to estimate dermal absorption.
Typically there is limited data and complexity is also that formulations can contain skin penetration enhancers, whereas some specific small nitrosamines can be activated on skin by light (assuming a full route of administration-specific risk approach might be expected if you go this route?).
There is also Franz 1993 on the absorption of NDELA, based on this SSCS assumes 65% dermal absorption for NDELA (so much higher). NDELA is hydrophilic, it is small enough to pass through the stratum corneum, especially when aided by surfactants or solvents. TABLE OF CONTENTS
Data is limited (not only on the absorption, but the overall scenario), especially for NDSRIs, and therefore not considered in risk assessment typically/defaulting to oral approach/full bioavailability.
I personally interpret the room for exceptions as needing nitrosamine/NDSRI-specific and matrix-specific absorption data being presented.