Thanks @kpcross for posting the update.
24-Mar-22:
Update to guidance on root causes and risk factors for nitrosamine contamination (Q&A 4) and on policy for confirmatory testing (Q&A 8) and dossier requirements (Q&A 15) to allow testing of intermediates, raw materials or API under certain circumstances.
20-May-22:
New Q&A 20 providing clarifications on what are the regulatory steps for dealing with scenario A cases and update Q&A 10 with new AIs (Nnitrosomethylphenidate, N-nitrosopiperidine, N-nitrosorasagilene, 7-Nitroso-3-(trifluoromethyl)-5,6,7,8-tetrahydro[1,2,4]triazolo-[4,3-
a]pyrazine, N-nitroso-1,2,3,6-tetrahydropyridine, Nnitrosonortriptyline, N-methyl-N-nitrosophenethylamine) and guidance on use of Ames test.
Q&A 8
“If a product is available in multiple strengths of the same dosage form with the same risk factors
applicable to each, then testing could be rationalised by testing only the worst-case scenario strength”
“During development of an analytical method, a reference standard of the relevant nitrosamine impurity is generally needed. If, despite extensive efforts, it becomes apparent that the relevant nitrosamine impurity cannot be synthesized, then this could be an indication that the nitrosamine either does not exist or that there is no risk of it being formed. . This should be justified thoroughly on a case by case basis according toappropriate scientific principles. The justification could include relevant literature, information onstructural/stereo-electronic features and reactivity of the parent amine, stability of the nitrosamine and experimental data to illustrate the efforts made to synthesize and to analyse the impurity. The justification should be documented in the risk assessment in the MAH’s pharmaceutical quality system”
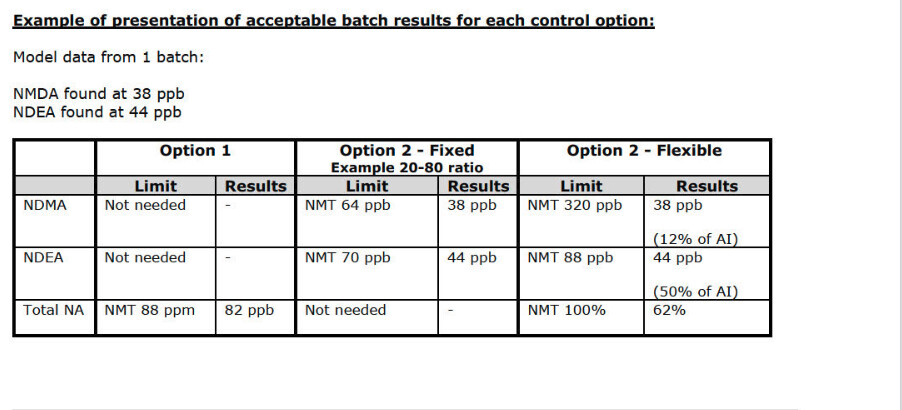
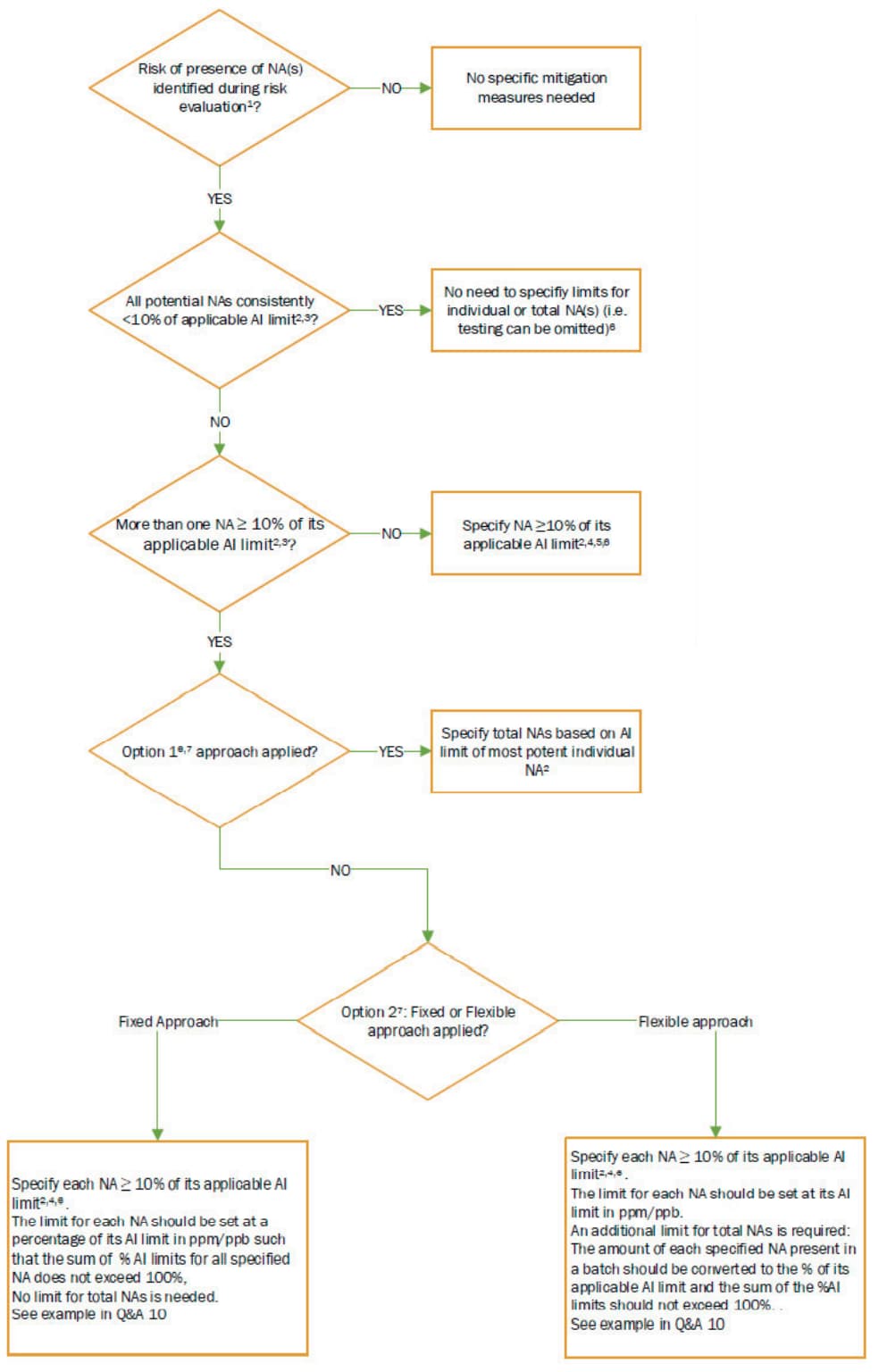
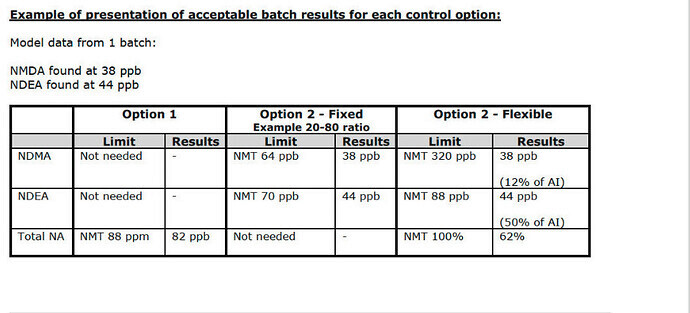
Q&A 10
At present, negative in vitro bacterial reverse mutation tests are not accepted by the EU network and international regulators as sole evidence for lack of mutagenic potential for nitrosamines and
classification as Class 5 impurities according to ICH M7. This is because some nitrosamines, which have elicited negative tests, have been shown to be carcinogenic in vivo and there are concerns that experimental conditions such as choice/concentration of solvent and metabolic activation system are not optimal for formation of activated species extracellularly which may also not be stable enough to reach DNA. Taking these concerns into account, a well conducted GLP-compliant in vitro bacterial reverse mutation test performed according to the OECD Guideline 471 and the concerns above can be used as part of a weight of evidence approach, but additional supporting evidence would be required to classify a nitrosamine as a Class 5 impurity. The EU network and international regulators, are working to ascertain if conditions for the in vitro bacterial reverse mutation test can be optimised for assessment of nitrosamine mutagenicity and determine how an optimised test can be used to decide on the need for additional tests and control options.
Q&A 20
In case of identification of one or more N-nitrosamine exceeding the AI in the finished product, or in case that the sum of all detected N-nitrosamines exceeds the 1 in a 100,000 lifetime risk (scenario A), the following steps are taken in order to protect public health and ensure availability of critical medicines:
• A lead authority is identified as responsible for reviewing the information available and for
providing the (preliminary) assessment of the case. The lead authority is selected as outlined in
chapter 5.1.
• The Rapid Alert Network (RAN) and the availability Single Point Of Contacts (SPOCs) are informed
in order to determine the criticality of the product (in accordance with Criteria for classification of critical medicinal products for human and veterinary use).
• The feedback from RAN and availability SPOCs is taken into account by the lead authority when
providing the preliminary recommendations on any interim or eventual required market actions
and on the acceptability of corrective and preventive actions proposed by the MAH.
• The Incident Review Network (IRN) is consulted in order to facilitate the exchange of information and to evaluate whether additional measures are needed or whether a different regulatory pathway is warranted.
• If market actions are recommended, each National Competent Authority (NCA) will follow up in
accordance with their national procedures and depending on the criticality of the product for their markets. The LTL concept or the use of interim limits may be considered by the lead authority and NCAs on a temporary basis for market action purposes in case of a critical product. Please refer to chapter 3.2.1.1.