Continuing the safety discussion, we learned about this new publication from @jbercu Bercu at al “Acceptable Intakes (AIs) for 11 Small molecule N-nitrosamines (NAs)”
Abstract
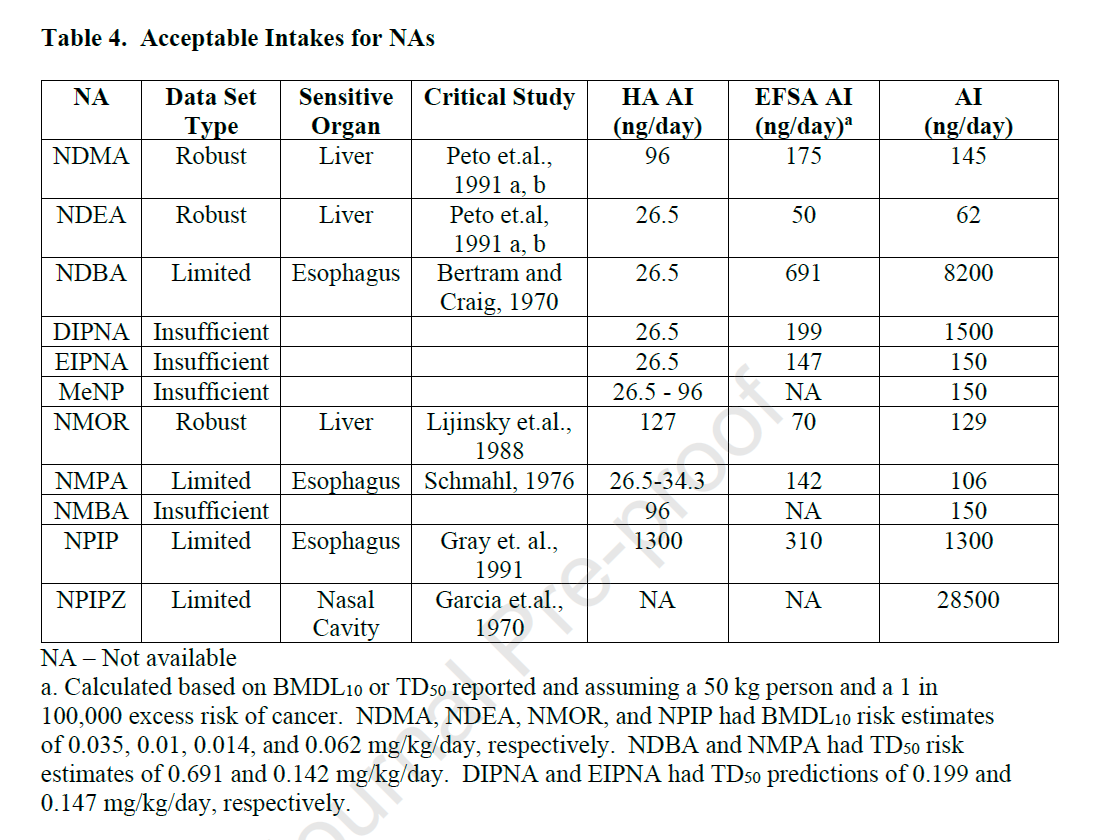
Low levels of N -nitrosamines (NAs) were detected in pharmaceuticals and, as a result, health authorities (HAs) have published acceptable intakes (AIs) in pharmaceuticals to limit potential carcinogenic risk. The rationales behind the AIs have not been provided to understand the process for selecting a TD50 or read-across analog. In this manuscript we evaluated the toxicity data for eleven common NAs in a comprehensive and transparent process consistent with ICH M7. This evaluation included substances which had datasets that were robust, limited but sufficient, and substances with insufficient experimental animal carcinogenicity data. In the case of robust or limited but sufficient carcinogenicity information, AIs were calculated based on published or derived TD50s from the most sensitive organ site. In the case of insufficient carcinogenicity information, available carcinogenicity data and structure activity relationships (SARs) were applied to categorical-based AIs of 1500 ng/day, 150 ng/day or 18 ng/day; however additional data (such as biological or additional computational modelling) could inform an alternative AI. This approach advances the methodology used to derive AIs for NAs.
DO NOT miss the supplemental information where the toxicological data was review and condensed in monographs following the same format as the ICH M7 addendum
The HA AI for many NAs with limited data is 26.5 ng/day, based on a read-across to NDEA. A change to the NDEA AI could have a significant impact on other AIs that were read-across to this compound.
The revised NDEA acceptable intake (AI) of 62 ng/day, considering the most sensitive site and tumor type, suggests a downstream impact on other limits. This prompts us to question the potential consequences of adjusting the AI for NDEA on other AIs that have been established based on read-across to this compound.
Furthermore, the paper raises an important point regarding the use of more mechanistic and metabolism data in read-across methodologies, particularly in the context of defining AIs for NDSRIs. These impurities often belong to a novel chemical space and exhibit different molecular characteristics and metabolic behaviors compared to small molecule NAs. The current default AI of 18 ng/day for NDSRIs is based on small molecule NAs that are readily metabolized into toxic species. However, the larger molecular weight and unique chemistry of NDSRIs may impede metabolism around the alpha-carbon position, necessitating a re-evaluation of the default AI.
From my modest point of view . They are a little optimistic to “save the furniture”:
I am surprised that more references of such a conservative character (that is, very high levels) such as the WHO or the IARC are not cited for the NDMA
or profiles as avant-garde as the state of California (low permissibility).
Just see NDMA that is widely studied… Remember that for water the std is 100 ng/L for WHO and California I think it drops to 10ng/L (also Germany¿?)
It seems to me that there is enough evidence to propose 2 scenarios for us:
Long-term and short-term drugs
Benefit risk and alternatives
I believe that it is necessary to defend not to make shortages of medicines but the risk affects all industries. There is no use just raising the tolerance because it suits me.
I think we are more exposed than we want to think. (Globally as humans)
… even more so if nitrite is allowed as a preservative (E250)…
I have a query related to NMPEA (AI limit - 8 ng/day as per EMA update). The authors suggest that the AI limit should be 40.1 ng/day citing Woolley et al. 2023.
This reference is of a poster presented in SOT 2023, which cites the Lijinsky et al. 1982 paper.
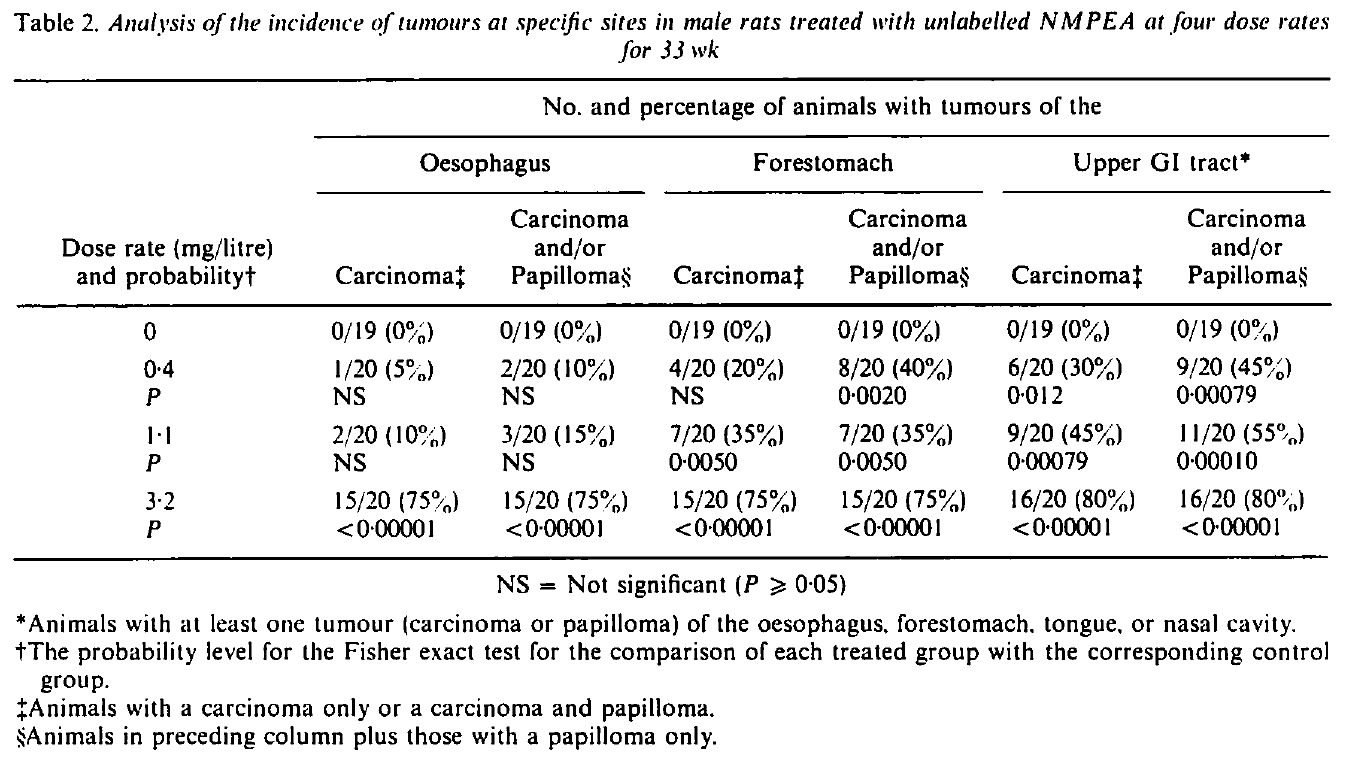
The argument of Bercu et al. 2023 is that the TD50 of the most potent organ site should be considered instead of the harmonic TD50. For NMPEA, the TD50 of the Upper GI tract was used to derive the AI limit, where as, the Lijinsky paper says esophagus is the most potent site. Based on TD50 of esophagus the AI limit comes to 40.1 ng/day.
The below table is data from the Lijinsky paper. In this the number and percentage of animals with tumours appear to be higher and significant in Forestomach than the esophagus. Hence, I want to understand on what basis the esophagus is being considered as the most potent site? Should TD50 value of forestomach be considered to derive the AI limit?
As per snapshot shared, it looks Forestomach is more sensitive than Oesophagus for NMPEA in rats for 33 weeks treatment. You may be correct. However, I have following observations:
Forestomach tumors in rats might not be relevant to humans!
If you pick lowest tested dose 0.4 mg/L for 104 weeks (the longest duration available), oesophagus looks more sensitive than forestomach with total incidence of with 8/20 for oesophagus and 5/20 for Forestomach.
If you consider entire range of doses tested 0.4 to 115 mg/L- Oesophagus looks more sensitive than forestomach.
I am in opinion, that might have led to @jbercu and team to conclude like this in the recent article published. May be @jbercu and rest all could add more clarity and correct me if i am incorrect.
Regardless, of above discussion, I am in opinion still harmonic Lhasa TD50 value holds good because the way NMPEA has resulted tumors in wide organs when tested at wide dose range and pertinently the lowest tested dose for 104 weeks resulted fair amount of tumors in most of the organs. Additionally, if we considered labelled NMPEA treatment as separate studies and the resulting tumors of it, it would be worthy enough to select harmonic mean TD50. Hope Lhasa derived this TD50 considering all the data. @David - can add more clarity in this aspect. I am not the expert!
EMA used Harmonic mean TD50 to represent nitrosamines in descending order of potency
Despite of above discussion, I still respect the attempt by @jbercu and team on recent publication on 11 small nitrosamines and though process to think on choice of sensitive organ TD50. I agree to some extent with their attempts does really a nitrosamine like NMPEA should be controlled at level of 8 ng/day!!
The general problem with harmonic mean TD50s is that they can be biased by low-quality studies that have unreliable but significantly different results (the 4000 rats of Peto et al have essentially the same weight towards the harmonic mean as a 5-rat single dose study!): the use of the most sensitive organ in the most robust study is therefore preferred, giving a much more robust answer (per M7 guidance and others). This is why there are differences between the values in current guidance for e.g. NDEA - where the harmonic mean was chosen as a matter of expediency (I assume) - and the value derived from the detailed, time-consuming analysis that we did in @jbercu et al, time which health authorities did not have when control limits were urgently needed for NDEA.
For NMPEA, the question is a bit different - it’s which row of the detailed data should be used. The 8 ug/kg/day TD50 comes from grouped “upper GI tract” results, which (a) includes the non-human-relevant forestomach and (b) is grouped tissues, rather than the most sensitive organ - the most potent single organ is the oesophagus at 40 ug/kg/day as discussed.
For the observation from @sushantkamath that looking at specific tested doses the forestomach may be more potent, that is one of the reasons it is critical to have multiple doses in a study and a good number of animals - it’s not the exact values at a specific tested dose that matter, which are subject to biological variability and have significant error bars, but rather the dose-response curve as a whole. This can be abstracted to the TD50 value (or other metrics such as benchmark dose), and it is clear from this that the oesophagus results are much more potent than the forestomach… as an aside, both oesophagus and forestomach show a reduction in tumor rates at higher doses. Lhasa Carcinogenicity Database has the calculated TD50 values.
I understand. Makes more sense. I had the privilege of meeting @conudel Dr. Nudelman today and his response was the same. Also, had the opportunity to listen to his talk on the new EMA update.
Hello,
Do you have any experience with regulatory authorities and how they respond to this approach of calculating the AI for NDEA? Has anyone used this approach or LTL approach to calculate and present the NDEA limit in regulatory purposes?
I shared the example of Entacapone. According to the document, LTL is applied to NDEA. As the PMDA shared the information related to the voluntary recall, the interim AI seems valid.
However, I am sorry I could not understand whether LTL applies to all nitrosamines in Japan. LTL can apply to NDEA at least, according to the document. We think the application of LTL is justified on a case-by-case basis.
Thanks @Yosukemino. Yeah the fact is LTL is scientifically appropriate to use in some cases. But Regulatory agencies allow only on case-by case basis despite of its merit in applicable cases!