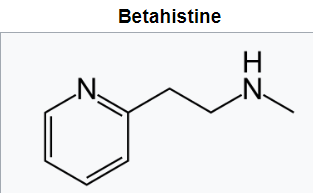
Recently it has been came to the notice that N-nitroso betahistine is one of the NDSRI in the betahistine formulation whose limit has not been defined by any of the regulatory authority.
Could any one suggest any AI limit based on the read across approach or literature based or any other leads?
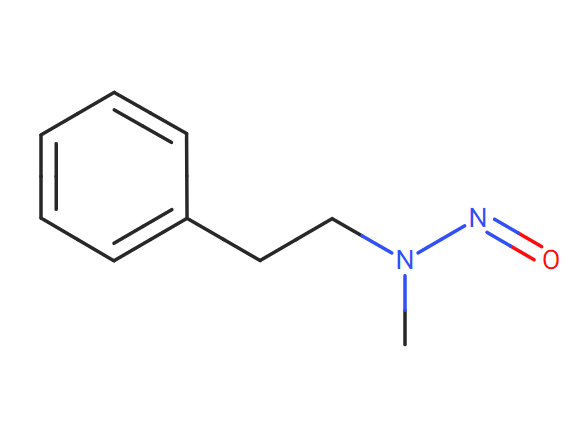
I would take N-Methyl-N-nitrosophenethylamine, NMPEA (13256-11-6) limit of 8 ng/day as the closest one and taking into account NMPEA is in EMA guidelines. Therefore, for me that means that the available carcinogenic data was considered robust enough for the agency.
@sumitkumarjain@Diego_HM
Dear both,
As per guidances & controlled approach, if there is no AI limit for any NNA, then we can use default value 18ng/ day or 26.5 ng /day, if still it is not controlling then need to evaluate AI limit by SAR. Prove it and get approval from agency to confirm the same.
However, for intial risk assessment to start the activity you can proceed with default value.
I agree with your comment Nilesh. However, lets put the case that the nitrosamine was detected above 18 ng/day or even 1.8 ng/day. I am pretty sure than when communicating to the Health Authority and an specific AI is stablished it will be for NMPEA or similar if there is other better analog. I believe that is what happened with N-Nitrosonortriptyline.
Is more a matter of preventive measure, because if a lower limit is defined by the agencies you will then come up with the topic of retesting and all the activities needed for that.
Additionally, I think is worth mention that the 18 ng/day covers 95% of the data. Not all and what actually EMA says is:
@Diego_HM
Absolutely right,
First default value---- then Related analog AI value---- then SAR AI value---- finally need to take approval & confirms the same from the agency, to proceed ahead for invivo test
Thanks for your responses. Of course, default value 18ng/day would be the proposal to the Authority. It seems the agency is aware of the higher level observed in the drug product and might have agreed internally with the limits to be assigned but would like researcher and industry to provide more data before the publication of the final limit.
Hi, all.
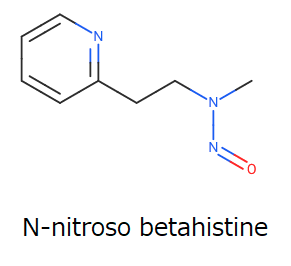
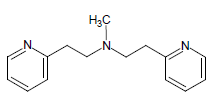
It is an interesting thread. To understand the topic deeply, I add the figure of N-nitroso betahistine.
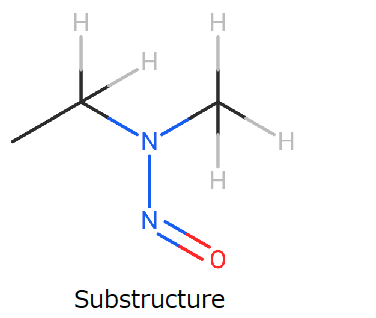
When I searched for analogs on LCDB substructure search with the following figure, an appropriate surrogate was not found, except for NMPEA.
That is why I support @Diego_HM’s suggestion. If less than 10% of 8ng/day is confirmed, the betahistine will be free from nitrosamine confidently in most cases. It is a fantastic scenario!!
For other officially used surrogates, please see the following post.
@Yosukemino I beleive the structure @Diego_HM was referring to is N-Nitroso-N-methyl-2-phenylethylamine (CAS 13256-11-6) TD50 0.00797 mg/kg/day, right?
Is there any correlation between the amount of nitrite present in the excipients and the potential for nitrosation of NDSRI (N-nitroso betahistine) under acidic condition to get some theoretical values of results in ppm. Betahistine contains a tertiary amine and alpha hydrogen and seems queries are more specific towards the potential of nitrosation of the drug substance.
Here is another one which is one of the probable impurity in betahistine and seems to be the potential source to form N-nitroso N-methyl-2-(pyridin-2-yl)-N-[2-(pyridin-2-yl)ethyl]ethanamine. Not sure whether to consider this under nitrosamine assessment as the same is controlled in the BP monograph with 2% limit.
Any structural analog suggestions for this impurity to apply read across approach?
Thank you for asking a good question, @sumitkumarjain. Betahistine contains a secondary amine and it is more reactive than a tertiary amine.
EFPIA workflow describes the risk assessment of the tertiary amine as follows;
Tertiary amines are significantly less reactive than secondary amines (reports of > 1000 fold lower reactivity) and require an additional de-alkylation step, making their nitrosation in solid state very unlikely. Certain tertiary amines where nitrosation could lead to class 1 low MW nitrosamines could, in certain instances (e.g. where the reactivity towards nitrite is enhanced by particular structural features), lead to an increased propensity towards nitrosation and should be considered as higher risk. Tertiary amines would generally be considered negligible risk given the mild conditions processing conditions would not be expected to lead to a nitrosamine.
Hi Sumitkumarjain
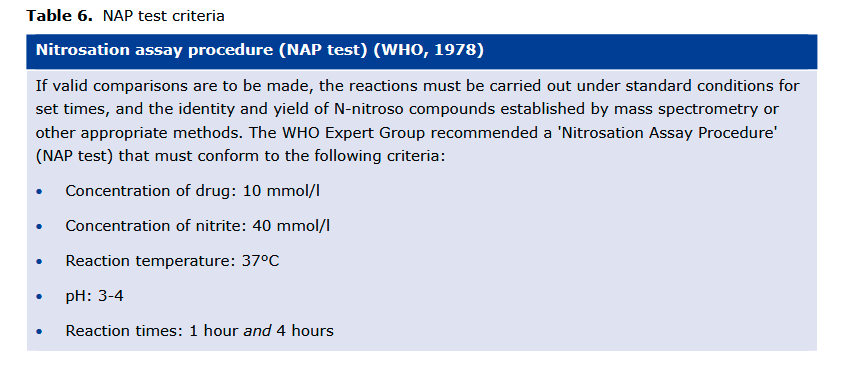
99.9% conversion rate after being incubated at 37°C for 4 h with an API concentration of 10 mmol/l in a 40-mol/l sodium nitrite solution at pH 3.5 (with 1 mol/l hydrochloric acid). The pH was adjusted in the sodium nitrite solution, measured (pH 3.5 ± 0.5), and corrected if necessary after the addition of sample material. https://onlinelibrary.wiley.com/doi/full/10.1002/ardp.202100435
How to move forward to assessment of nitrosamine (NDSRIs) as contained of tertiary amine in impurity/API OR tertiary amine containing API is considered as low risk for NDSRIs formation.
EFPIA mentioned certain tertiary amines where nitrosation could lead to class 1 low MW nitrosamines could, in certain instances (e.g. where the reactivity towards nitrite is enhanced by particular structural features), lead to an increased propensity towards nitrosation. This very common alkyl dimethyl amine may have the potential.
To understand the reactivity of tertiary amines, the NAP test is helpful. I will search for good literature.
@Yosukemino : the question is still there, "how to conclude the risk when there is tertiary amine in structure? what justification will suffice the requirement for not to perform confirmatory testing?
or Should we opt for performing confirmatory testing regardless secondary or tertiary amine?
Thank you for asking, @Chirag. I think it depends on the possible risk of nitrosamines contamination. You can take the AI limits of nitrosamines, the MDD of the products, manufacturing processes, the amounts of nitrite in excipients, pKa of amines, and other mitigating factors such as pH into consideration. The example demonstrated by Dr. Urquhart is helpful.
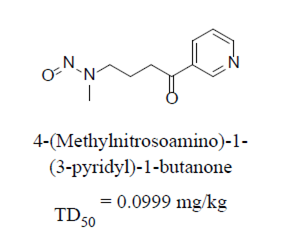
Back to N-Nitroso-Betahistine closest surrogate, wouldnt be possible to think of this one?:
This compound called NNK was already used as point of departure for nitroso duloxetine and fluoxetine both published in Q&A.
Compared to above mentioned NMPEA surrogate it has pyridine heterocycle, same as betahistine has: