Hi, everyone
I am an analyst.
Because of Inderal-LA (Propranolol Hydrochloride) capsules Pfizer recalls, I will study the nitroso-Propranolol in my drug product.
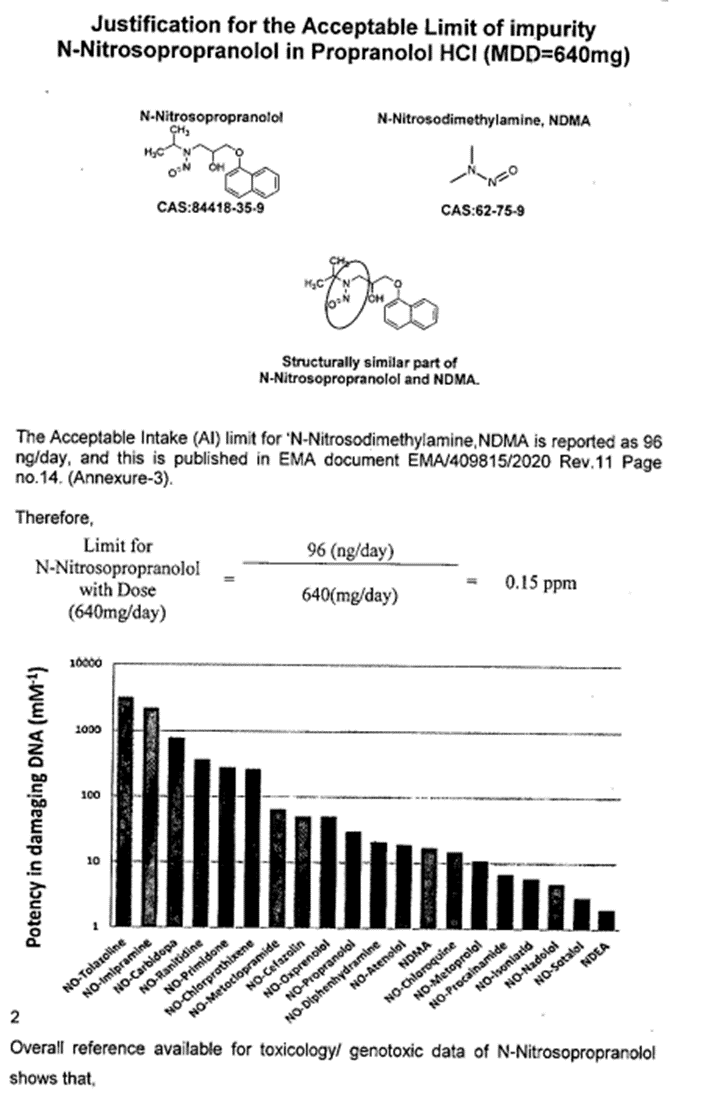
The API vender provide me the report explaining the potency of DNA damaging were similar between NDMA and NO-Propranolol and the acceptance intake should be similar to NDMA, 96 ng/ day.
Do it be correct?
Hi,
the carcinogenic potency of all the beta-blockers is still under discussion.
In Europe. Very recently EMA aknowlegded that:
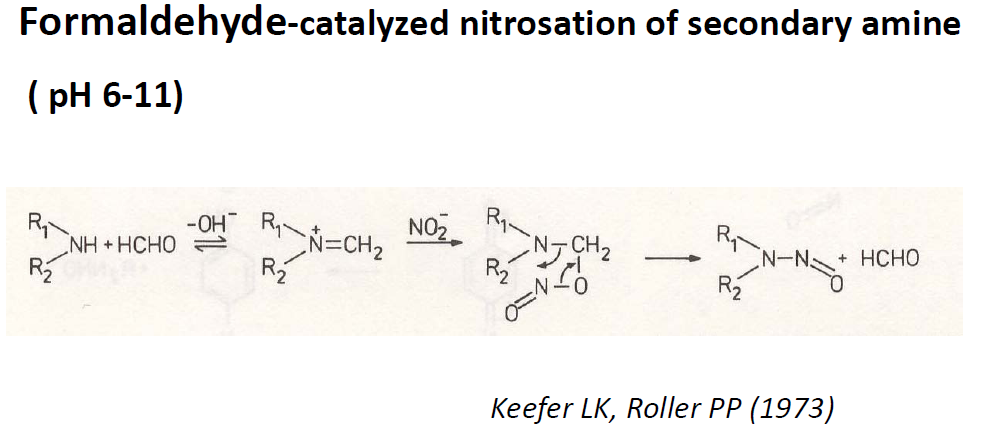
All the β-blockers have a secondary amine that can undergo nitrosylation under suitable conditions to give the N-nitrosamine derivative.
• Besides carvedilol and nebivolol, all the other β-blockers have bulky (isopropyl, isopropyl with further substitution, or tert-butyl) groups at the α-position to the secondary amine.
• Carvedilol and nebivolol have CH2 groups at both α-positions, however the substituents on both sides of the amino group are large/bulky groups that render considerable steric hindrance.
• It is very likely that these factors reduce the carcinogenic potency of any related Nnitrosamine however it is recognised that further investigation is needed to completely understand this
I remember that the position of each autority (EMA, TGA, U.S.FDA, KFDA, etc) may be different and each authority may accept the proposed limit or ask a tighter limit.
kind regards
The latest EMA Nitrosamine Implementation Oversight Group meeting discussed beta blockers specifically. The industry presentation slides are a must read for anyone working with Propranolol.
Unlike other NDSRIs, an experimental study is available for N-Nitrosopropranolol reported in 1983 by Ilene H. Raisfeld-Danse and Jack Chen from the State University of New York at Stony Brook, New York. As per the published literature, N-Nitrosoproranolol (NNP) is unlikely to be a carcinogen. Therefore, in my opinion, comparing NNP with NDMA is absurd.
Hi,
As per ICH M7 (R1) & Health Canada “Guidance on Nitrosamine impurities in medication”, In case there is no sufficient carcinogenic data is available for nitrosamine impurity, it is recommended to derive the limit from the comparison of the Structure activity relationship.
N-Nitrosodimethylamine, NDMA (CAS:62-75-9) is structurally similar to N-Nitrosoproporanolol hence limit of NDMA 96 (ng/mg) is considered with MDD 640 mg for US Market where limit for N-Nitrosoproporanolol is 0.15 ppm.
However for Europe market, approach of a temporary Al (t-Al) of 178ng/day (total nitrosamine) is adopted for defining the limit of N-Nitrosopropranolol in Propranolol HCl. This approach is outline in EMA Guidance EMA/409815/2020 Rev.14 under section 21, Page 26 of 28. Using this approach, limit is calculated for N-Nitrosopropranolol is 0.28 ppm.
Both limits are temporary limit and this limit may be revised in the future when a compound specific Al is established by competent authority.
I am really puzzled that NDMA has been used as a surrogate for N-nitroso-propanolol. I really doubt the BoH would accept that proposal. Or maybe I am wrong, but compare symple alkyl nitrosamines with this more complex compounds would be difficult to justify.
Please look at the previous discussion, regarding the Dobo paper and the materials from the EMA oversight group. Not only should the limit be substantially higher, a limit similar to NDMA would take the drug off the market. There is no path to achieve that limit.
it is important to put this into context. These are in vitro data and do not necessarily correlate with in vivo data. It is important that we have such data before we can draw definitive conclusions over potency.
@Naiffer_Host . I think the purpose of this publication is to clear the cloud of ambiguity surrounding N-nitroso propranolol (NNP). As per my observation, this is one of the NDSRI that has enough mixed opinions for genotoxicity in various publications.
To clear this- FDA made an attempt to address this by battery of in vitro assays. Again as @AndyT mentioned, we never know how well they co-relate to in vivo and then again co-relate to human health risk assessment.
It is interesting to note in the same publication- NNP was found to have lower mutagenicity when compared with NDEA and higher clastogenicity with same NDEA. So, i think more experimentation and analysis is required to arrive to the conclusion whether NNP is potent mutagenic and carcinogenic.