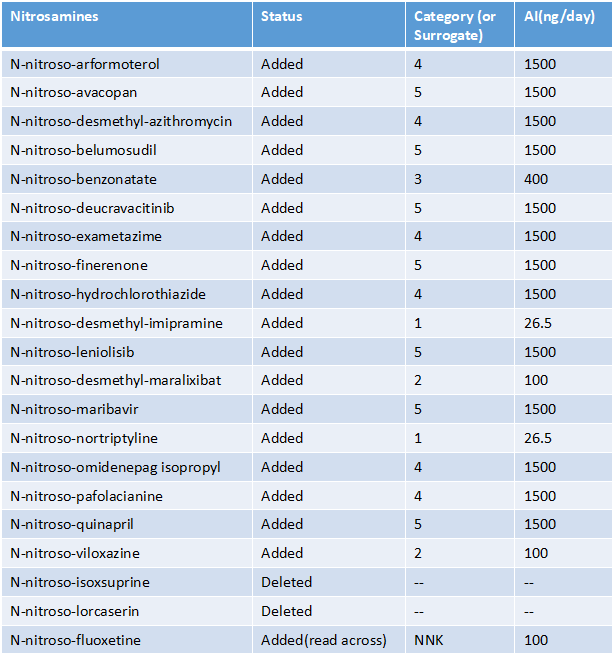
The FDA updated their list of published AIs yesterday, adding 19 compounds and deleting two. Some highlights:
Contrary to EMA, no change to nitrosovarenicline AI - still read-across to 37
Several in vivo negatives - quinapril, HCTZ, desmethyl-azithromycin - added to the list but as their CPCA category not as NMI (presumably implies a non-acceptance of in vivo negative data accepted by EMA/HC?)
Nitroso-fluoxetine read across to NNK
Nitroso-nortriptyline at CPCA category 1 rather than read-across to NMPEA (3-fold higher limit as a result)
I would be really be surprised that a -ive TGR is not enough to control impurities to ICH Q3A/B levels. What else could you do then do? There is a lot of effort to do TGRs and I do not know of cases of a -ive Ames being +ive in-vivo.
Also I see interesting that read-across from NMPEA are being eliminated. I would infer NMPEA do not have robust data or questionable current limit.
Finally, I wonder if in reality all the FDA list is based on positive cases or not. As for example, they have eliminated 2 nitrosamines. Would that mean they were not possible to be synthetised? I would not think so, that compounds do not seem special to avoid nitrosation. Then same question, why?
As always interesting to see each new update that comes.
Interestingly, the CPCA preamble was not followed (“where the carbon is not directly double bonded to a heteroatom (i.e., N-nitrosamides, N-nitrosoureas, N-nitrosoguanidines and other related structures are excluded)”) considering the assignment of a CPCA class 5 to N-nitroso-maribavir. I presume just a mistake, but the pseudonitrosamines topic still doesn’t seem fully closed (cf. EMA confirmed also that pseudonitrosamines are out of the call for review (so governed under ICH M7) besides being out of scope of CPCA).
I’m also surprised by the lack of acceptance of negative in vivo - it means that a drug with an Ames positive/in vivo negative cat 1/2 NDSRI impurity, perfectly able to be marketed in the rest of the world could easily, and arguably unnecessarily, be forced into the realms of market actions being taken, because reliable control below those limits is challenging even to measure, let alone to achieve, in many cases (or a two year carc study, and presumably US marketing suspended until that reads out, if the MAH even thinks it’s worthwhile doing…), whereas a negative in vivo should be able to show a lack of in vivo relevance of that Ames positive - one of the main reasons to follow a positive Ames up in vivo!
In terms of NMPEA, the data for the study, while multiple-dose, is otherwise a bit dubious for several reasons, including the use of a multi-organ line to set the 8 ng limit rather than the most sensitive organ, and the fact that the exposures were only for ~1/3 lifetime.
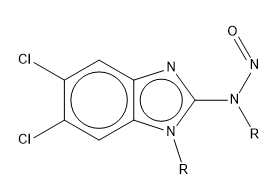
For maribavir, it depends how you define an aromatic bond vs a double bond - the double bond to heteroatom is in an aromatic ring, rather than being a formal double bond, so isn’t perceived as a true double bond in many cheminformatics toolkits, nor does it behave as a guanidine-like structure in this case, which was the intention of the exclusion - to remove the nitrosamide-like structures which can be abiotically hydrolysed to yield diazonium ions from the metabolism-dominated SAR of the CPCA. It can be visualised as the below delocalised form rather than having the explicit double bond:
On the N-nitroso-isoxsuprine and N-nitroso-lorcaserin deletion:
Lorcaserin is no longer a marketed API in the US since 2020 I believe, for isoxsuprine there was a stop distribution from FDA in 2021.
So from that perspective it could give a contradictory message to have the NDSRIs in the list.
Cidoxepin NDSRI was not removed, I understand this API was developed in the ’60 but never marketed, but here you probably have to read the entry as an isomer of the doxepin NDSRI (cis instead of trans double bond).
Ah, that almost certainly explains the removal - as well as some of the other inter-agency discrepancies in which compounds are covered, potentially - thanks!
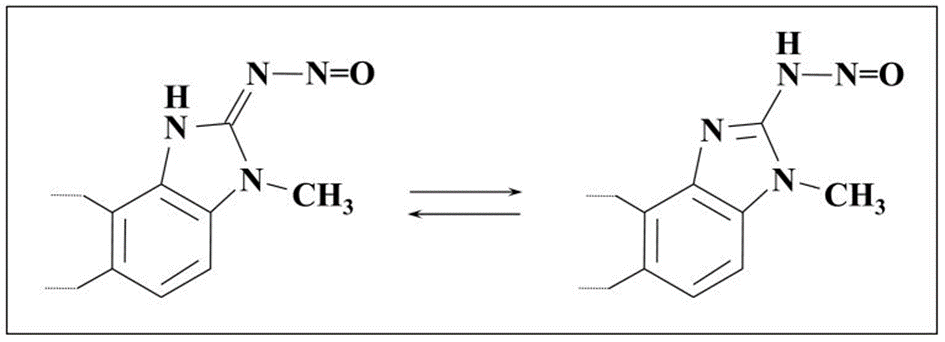
Chemically speaking it should at least fall under the “other related structures” from the CPCA exclusion preamble. The preamble doesn’t speak about a double bond in general, but as double bond linked to a heteroatom, which are typically linked to electron delocalization (tautomerism), as are the examples specified. That there is an extra factor to electron delocalization (being the aromatic system rather than a simple guanidine sensu stricto), doesn’t seem a reason to me to exclude it from a chemical perspective. (Maybe such structures are also not in the 84 nitrosamines of the CPCA model data set often (haven’t rechecked the presence of nitrosated 1H-Benzimidazol-2-amines in potency databases though), which we still don’t know fully unfortunately in order to build the model independently). After all the exclusion criteria are described chemically and not biologically and not as a numerus clausus system considering “other related structures” is mentioned, so one could dare to see the 1H-Benzimidazol-2-amine as excluded. Cf. also the tautomers of N-nitrosobenzimidazoles structures and research showing they mostly exist as nitrosoimino tautomers (for the specific case where the N-substituent is H though).
I agree though the intention of the exclusion was probably to exclude specific structures which have no link with how the model was designed and/or for which classic alpha-hydroxylation is not likely/possible but where at the same time other mutagenicity mechanisms could play (and lack of alpha-CH2 is just corrected by hydrogen scoring and not CPCA exclusion). The biological mechanism of acetylation and deacetylation of the nitrosated 1H-Benzimidazol-2-amines towards a diazonium is maybe not sufficiently different to read CPCA exclusion in it (although this is what I’m doing), but at the same time the preamble of FDA says “the approach assumes alpha-hydroxylation mechanism of metabolic activation is responsible of metabolic activation” (for many nitrosamines). And alpha-hydroxylation is not the rationalised mechanism for mutagenicity for the full group so can you include them (depending on N substituent). More transparency and a way to reconstitute the building of the CPCA model and limits still feels helpful. (So glad to see also remarks on lack of transparency how certain CPCA classes were calculated in the recent paper Regulatory Toxicology and Pharmacology 145 (2023) 105505 you contributed to).
Hello team, your input is highly appreciated. I’m looking for any updates regarding the FDA’s guidance on NDSRIs. The guidance suggests that if NDSRIs weren’t considered in previous risk assessments, manufacturers and applicants should review the risks within three months of the guidance’s publication. The recommended deadline for completion is November 1, 2023, as part of an overall risk management strategy.
I’m wondering if the FDA is requesting a theoretical NDSRI assessment and if it’s feasible for all drug products to meet this strict deadline.
Do we have any information on whether this deadline might be extended? Because to evaluate the NDSRI in a drug product we need a thorough assessment of drug product components, manufacturing method etc. @Naiffer_Host
Table 1 & 2-mentioned Tertiary amines NDSRIs N-Nitroso desmethyl impurities but none of them were N-Nitroso desethyl impurities in all the listed 263 and updated 6 impurities.
Any information on the tertiary amines with diethyl group please let me know.
One of the member posted similar query on Aug 2022 but no one replied.
I want to inform you of the update of the FDA list. In the rev.2, N-nitroso-ciprofloxacin was transferred from the read-across list to the CPCA list. And N-nitroso-atomoxetine was transferred from the CPCA list to the read-across list.
2
N-nitroso-ciprofloxacin
Added to Table 1
12/1/2023
2
N-nitroso-ciprofloxacin
Deleted from Table 2
12/1/2023
2
N-nitroso-atomoxetine
Deleted from Table 1
12/1/2023
2
N-nitroso-atomoxetine
Added to Table 2
12/1/2023
N-nitroso-ciprofloxacin: from “Pending” to “Category4 (1500ng/day)”
N-nitroso-atomoxetine: from “Category1 (26.5ng/day)” to “read-across from NNK (100ng/day)”